

Ordinary standard of care includes dietary restrictions and
lifestyle changes, stress-management techniques, In some severe cases, medicine
for pain, diarrhea, or constipation is needed to give the IBS patient
comfort. There are also other natural treatments for IBS. The
following video details some more holistic solutions for IBS:
After serious diagnoses are ruled out, what could be another source of these IBS symptoms?
Small intestine bacterial overgrowth (SIBO) is a condition in which abnormally large numbers of symbiotic bacteria are present in the small intestine. SIBO is a common cause of IBS – in fact it is involved in over half the cases of IBS and as high as 84% in one study using breath testing as the diagnostic marker.1,2 Eradication of this overgrowth leads to a 75% reduction in IBS symptoms.4 Bacterial overgrowth leads to impairment of digestion and absorption and produces excess quantities of hydrogen and/or methane gas. These gases are not produced by human cells but are the metabolic product of fermentation of carbohydrates by intestinal bacteria. When symbiotic bacteria (oral, small intestine or large intestine) multiply in the small intestine to the point of overgrowth, IBS is likely to occur in that patient. Hydrogen/methane breath testing is the most widely used method of testing for this overgrowth. hydrogen/methane breath testing is the most common method of assessing SIBO. Instrumentation is available from Quintron Instrument Company in Milwaukee, Wisconsin. It provides a device called the Breathtracker, which is used to measure these gases following a 24-hour prep diet and an overnight fast. Stool sample testing is of no value in diagnosing SIBO.
Symptoms of SIBO include:
•
bloating/ abdominal gas
•
flatulence, belching
•
abdominal pain, discomfort, or cramps
•
constipation, diarrhea or a mixture of the two
•
heartburn
• nausea
•
malabsorption: steatorrhea, anemia
• systemic
symptoms: headache, joint/muscle pain, fatigue, rosacea
Other diseases associated
with SIBO include hypothyroidism, lactose intolerance, Crohn's disease,
systemic sclerosis, celiac disease, chronic pancreatitis, diabetes with
autonomic neuropathy, fibromyalgia and chronic regional pain syndrome, hepatic
encephalopathy, nonalcoholic steatohepatitis, interstitial cystitis, restless
leg syndrome, and acne rosacea.5–17
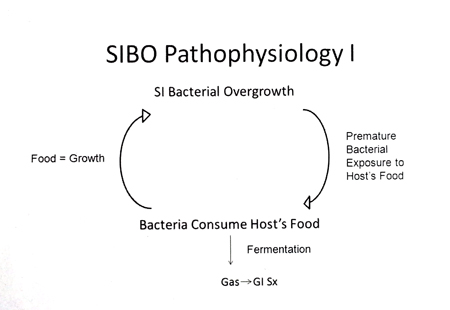
There are two main
pathophysiological issues involved in SIBO and related to IBS.
First, bacteria
can ferment food meant for the host simply by their inappropriate location in
the small intestine, which allows them premature exposure to host nutrition.
Bacterial fermentation produces hydrogen and/or methane gas. Bacterial gas
leads to the IBS symptoms of bloating, pain, altered bowel movements,
eructation and flatulence (Figure 1). The quantity of gas may be extensive,
causing bloating/distention.26 Excess gas can then exit the body as
flatulence or eructation. The intestines are sensitive to pressure and
therefore the pressure of distention can lead to abdominal pain. In addition,
visceral hypersensitivity, a feature of IBS, may create a lower threshold for
pain/discomfort and a hyperresponsiveness of muscular contraction in response
to the gas, leading to cramps in some.27,28 The gases also affect bowel
motility with hydrogen having a greater association with diarrhea and methane
having an almost exclusive association with constipation.29,30 Methane has
been shown to slow gastrointestinal motility by 59% in animal studies, and the
volume of methane overproduction correlates with the severity of
constipation.31,32 Therefore when both hydrogen and methane are present,
diarrhea, constipation, or a mixture of both can be present based on the
relative amounts of gases.29 The bacterial consumption and uptake of host
nutrients, such as B12 and iron, can lead to macrocytic and/or microcytic
anemia or chronic low ferritin, in addition to general malabsorption and
malnutrition in more severe cases.8,33 The increased motility of diarrhea
may also induce malabsorption. Finally, continuous fermentation of host
nutrition by repeated exposure to daily meals, perpetuates bacterial overgrowth
and its symptoms, creating a vicious cycle (Figure 1).
Figure 1
Second, bacteria damage the
digestive and absorptive structure and function of the small intestine. This
occurs because, unlike the large intestine, the small intestine is not designed
for large colonization. The damage leads to both gastrointestinal and systemic
symptoms. Key damaging factors are: bacterial deconjugation of bile, which
creates fat malabsorption (steatorrhea, fat-soluble vitamin deficiency);
bacterial digestion of disaccharide enzymes, which furthers carbohydrate
malabsorption, fermentation, and gas; and increased intestinal permeability
(leaky gut), which leads to systemic symptoms and allergies.34–38
PREVENTION AND HOLISTIC
TREATMENTS FOR SIBO
An important protective
mechanism against SIBO is proper small intestine motility because stasis
promotes bacterial growth.18 Also key in prevention is normal gastric HCl,
pancreatic, and gall bladder secretions, since hydrochloric acid, enzymes, and
bile are bactericidal/static.19
Hydrochloric acid or herbal
bitter supplements encourage hydrochloric acid (HCl) secretion and may be used
to decrease the load of incoming bacteria.39 When considering HCl
supplementation, Heidelberg testing for HCl level and function is the gold
standard and allows individualization of dosing.
Probiotics are a
controversial intervention in SIBO because lactobacilli have been cultured in
SIBO and there is concern about adding to the bacterial overload, particularly
in this situation of dysfunctional MMC.25 Despite this, the few studies
that have focused directly on SIBO have shown good results, with a SIBO
eradication rate of 47% from Bacillus clausii as the only treatment, and a
clinical improvement rate of 82% from Lactobacillus casei and plantarum,
Streptococcus faecalis, and Bifidobacter brevis (Bioflora) as the only
treatment.40.41 Probiotic yogurt containing Lactobacillus johnsonii
normalized cytokine responses – reducing the low-grade chronic inflammation
found in SIBO, after 4 weeks.42
A key point for the use of probiotic
supplements in SIBO is to avoid prebiotics as main ingredients. Prebiotics
are fermentable food for bacteria that can exacerbate symptoms during active
SIBO and encourage bacterial growth post SIBO. Common prebiotics found in
probiotic supplements include FOS (fructooligosaccharide), inulin,
arabinogalactan, and GOS (galactoligosaccharide). Prebiotics may be tolerated
in small amounts used as base ingredients, but this depends on the individual.
Brush border healing
supplements may be given to assist the repair of small intestine tissue. While
mucilaginous herbs are traditionally employed for this purpose (licorice,
slippery elm, aloe vera, marshmallow), their use is controversial post SIBO,
due to their high level of mucopolysaccharides, which could encourage bacterial
regrowth. Specific nutrients that have been used to repair damaged samll
intestine tissue include colostrum: 2–6 g q.d., L-glutamine: 375 mg–1500 mg
q.d., zinc carnosine: 75–150 mg q.d., vitamins A and D, often given as cod
liver oil: 1 Tbs q.d., curcumin: 400 mg–3 g q.d., resveratrol: 250 mg–2 g q.d.,
glutathione (oral liposomal): 50–425 mg q.d. or glutathione precursor
N-acetylcysteine 200–600 mg q.d. Supplements are given for one to three months,
though may be continued long term for general benefit.
The recommended diet is
(Specific Carbohydrate Diet or Gut and Psychology Syndrome Diet) for all SIBO
patients. 41,42,43 Since bacteria use carbohydrates as their energy source and
ferment them to gas, a low-carbohydrate diet can directly reduce symptoms by
decreasing the amount of gas produced.44Reducing carbohydrates may also reduce
the overall bacterial load as the food supply shrinks, though formal studies to
validate this are lacking. These diets decrease polysaccharides,
oligosaccharides, and disaccharides by eliminating all grains, starchy
vegetables, lactose, sweeteners other than honey, and in the beginning, beans.
Many patients experience a rapid and significant decrease in symptoms after starting
a SIBO diet. The Specific Carbohydrate Diet (SCD) has been reported to have an
84% success rate for inflammatory bowel disease, a condition commonly
associated with SIBO.44,45
REFERENCES
1. Peralta S et
al. Small intestine bacterial overgrowth and irritable bowel syndrome-related
symptoms: experience with Rifaximin. World J Gastroenterol. 2009 Jun
7;15(21):2628–2631.
2. Lin HC et al. Small intestinal bacterial
overgrowth: a framework for understanding irritable bowel syndrome. JAMA. 2004
Aug 18;292(7):852–858.
3. Pyleris E et al. The prevalence of
overgrowth by aerobic bacteria in the small intestine by small bowel culture:
relationship with irritable bowel syndrome. Dig Dis Sci. 2012
May;57(5):1321–1329.
4. Pimentel M et al. The effect of a
nonabsorbed oral antibiotic (rifaximin) on the symptoms of the irritable bowel
syndrome: a randomized trial. Ann Intern Med. 2006 Oct 17;145(8):557–563.
5.
Lauritano EC et al. Association between hypothyroidism and small intestinal
bacterial overgrowth. J Clin Endocrinol Metab. 2007 Nov;92(11):4180–4184.
6.
Almeida JA et al. Lactose malabsorption in the elderly: role of small
intestinal bacterial overgrowth. Scand J Gastroenterol. 2008;43(2):146–154.
7.
Klaus J et al. Small intestinal bacterial overgrowth mimicking acute flare as a
pitfall in patients with Crohn's Disease. BMC Gastroenterol. 2009 Jul
30;9:61.
8. Marie I, Ducrotté P, Denis P, Menard JF, Levesque H.
Small intestinal bacterial overgrowth in systemic sclerosis. Rheumatology
(Oxford). 2009 Oct;48(10):1314–1319. Epub 2009 Aug 20.
9.
Rubio-Tapia A et al. Prevalence of small intestine bacterial overgrowth
diagnosed by quantitative culture of intestinal aspirate in celiac disease. J
Clin Gastroenterol. 2009 Feb;43(2):157–161.
10. Mancilla AC et al. [Small
intestine bacterial overgrowth in patients with chronic pancreatitis].Rev Med
Chil. 2008 Aug;136(8):976–980.
11. Ojetti V et al. Small bowel
bacterial overgrowth and type 1 diabetes. Eur Rev Med Pharmacol Sci. 2009
Nov–Dec;13(6):419–423.
12. Goebel A et al. Altered intestinal permeability in
patients with primary fibromyalgia and in patients with complex regional pain
syndrome. Rheumatology (Oxford). 2008 Aug;47(8):1223–1227.
13.
Gupta A et al. Role of small intestinal bacterial overgrowth and delayed
gastrointestinal transit time in cirrhotic patients with minimal hepatic
encephalopathy. J Hepatol. 2010 Nov;53(5):849–855.
14. Shanab AA et
al. Small intestinal bacterial overgrowth in nonalcoholic steatohepatitis:
association with toll-like receptor 4 expression and plasma levels of
interleukin 8. Dig Dis Sci. 2011 May;56(5):1524–1534.
15.
Weinstock LB, Klutke CG, Lin HC. Small intestinal bacterial overgrowth in
patients with interstitial cystitis and gastrointestinal symptoms. Dig Dis
Sci. 2008 May;53(5):1246–1251.
16. Weinstock LB, Walters AS,
Restless legs syndrome is associated with irritable bowel syndrome and small
intestinal bacterial overgrowth. Sleep Med. 2011 Jun;12(6):610–613.
17.
Parodi A et al. Small intestinal bacterial overgrowth in rosacea: clinical
effectiveness of its eradication. Clin Gastroenterol Hepatol. 2008
Jul;6(7):759–764.
18. Husebye E. The patterns of small bowel motility:
physiology and implications in organic disease and functional disorders. Neurogastroenterol
Motil. 1999 Jun;11(3):141–161.
19. Bures J. 2010 Small intestinal
bacterial overgrowth syndrome. World J Gastroenterol. 2010 Jun
28;16(24):2978–2990.
20. Pyleris E et al. The prevalence of overgrowth by
aerobic bacteria in the small intestine by small bowel culture: relationship
with irritable bowel syndrome. Dig Dis Sci. 2012 May;57(5):1321–1329.
21.
Williams C et al. Occurrence and significance of gastric colonization during
acid-inhibitory therapy. Best Pract Res Clin Gastroenterol. 2001
Jun;15(3):511–521.
22. Machado WM et al. The small bowel flora in individuals
with cecoileal reflux. Arq Gastroenterol. 2008 Jul–Sep;45(3):212–218.
23.
Khoshini R, Dai SC, Lezcano S, Pimentel M. A systematic review of diagnostic
tests for small intestinal bacterial overgrowth. Dig Dis Sci. 2008
Jun;53(6):1443–1454.
24. Pimentel M. Gut microbes and irritable bowel syndrome
[webcast]. July 20, 2012. GI Health Foundation. http://www.gihealthfoundation.org/coe/ibs/webcast/2012/july/MPimentel/?link=2012/
july/MPimentel&cme_proj_id=12&actionPage=topics/Gut_Microbes_and_
IBS/request-for-credit.cfm?cme_proj_id=12.
25. Bouhnik Y et al.
Bacterial populations contaminating the upper gut in patients with small
intestinal bacterial overgrowth syndrome. Am J Gastroenterol. 1999 May;94(5):1327–1331.
26.
Youn YH, Park JS, Jahng JH, et al. Relationships among the lactulose breath
test, intestinal gas volume, and gastrointestinal symptoms in patients with
irritable bowel syndrome. Dig Dis Sci. 2011 Jul;56(7):2059–2066. Epub 2011
Jan 15.
27. Elsenbruch S. Abdominal pain in irritable bowel syndrome: a review
of putative psychological, neural and neuro-immune mechanisms. Brain Behav
Immun. 2011 Mar;25(3):386–394. Epub 2010 Nov 20.
28. Pimentel M. A
New IBS Solution. Sherman Oaks, CA: Health Point Press; 2006.
29. Pimentel M,
Mayer AG, Park S, Chow EJ, Hasan A, Kong Y. Methane production during lactulose
breath test is associated with gastrointestinal disease presentation. Dig
Dis Sci. 2003 Jan;48(1):86–92.
30. Kunkel D et al. Methane on breath testing is
associated with constipation: a systematic review and meta-analysis. Dig
Dis Sci. 2011 Jun;56(6):1612–1618.
31. Pimentel M, Lin HC, Enayati
P, et al. Methane, a gas produced by enteric bacteria, slows intestinal transit
and augments small intestinal contractile activity. Am J Physiol
Gastrointest Liver Physiol. 2006 Jun;290(6):G1089–G1095. Epub 2005 Nov 17.
32.
Chatterjee S et al. The degree of breath methane production in IBS correlates
with the severity of constipation. Am J Gastroenterol. 2007
Apr;102(4):837–841.
33. Singh VV, Toskes PP. Small bowel bacterial overgrowth:
presentation, diagnosis, and treatment.Curr Treat Options Gastroenterol. 2004
Feb;7(1):19–28.
34. DiBaise JK. Nutritional
consequences of small intestinal bacterial overgrowth. Prac Gastroenterol.
2008;69:15–28.
35. Prizont R. Glycoprotein degradation in the blind loop
syndrome: identification of glycosidases in jejunal contents. J Clin
Invest. 1981 Feb;67(2):336–344.
37. Lauritano EC, Valenza V, Sparano L, et al.
Small intestinal bacterial overgrowth and intestinal permeability. Scand J
Gastroenterol. 2010 Sep;45(9):1131–1132.
36. Resnick C. Nutritional protocol
for the treatment of intestinal permeability defects and related conditions. Nat
Med J. March 2010.
38. Bowman, G. The Gut,
the Brain and the Functional GI Disorders. Functional Gastroenterology Seminar:
Level 1. Winter 2010, p. 19.
39. Gabrielli M, Lauritano
EC, Scarpellini E, Lupascu A, Ojetti V, Gasbarrini G, Silveri NG, Gasbarrini A.
Bacillus clausii as a treatment of small intestinal bacterial overgrowth. Am
J Gastroenterol. 2009 May;104(5):1327–8. Epub 2009 Apr 7.
40. Soifer LO,
Peralta D, Dima G, Besasso H. Comparative clinical efficacy of a probiotic vs.
an antibiotic in the treatment of patients with intestinal bacterial overgrowth
and chronic abdominal functional distension: a pilot study. Acta
Gastroenterol Latinoam. 2010 Dec;40(4):323–7.
41. Schiffrin EJ, Parlesak A,
Bode C, Bode JC, van't Hof MA, Grathwohl D, Guigoz Y. Probiotic yogurt in the
elderly with intestinal bacterial overgrowth: endotoxaemia and innate immune
functions. Br J Nutr. 2009 Apr;101(7):961–6.
42. Gottschall E. Breaking
the Vicious Cycle. Baltimore, ON: Kirkton Press Ltd.; 1994.
43.
Campbell-McBride N. Gut and Psychology Syndrome. Cambridge: Medinform
Publishing; 2004.
44. Ong DK, Mitchell SB, Barrett JS, et al. Manipulation of
dietary short chain carbohydrates alters the pattern of gas production and
genesis of symptoms in irritable bowel syndrome. J Gastroenterol Hepatol.
2010 Aug;25(8):1366–1373.
45. Nieves R, Jackson RT. Specific carbohydrate diet
in treatment of inflammatory bowel disease.Tenn Med. 2004 Sep;97(9):407.
This an informative and helpful post - so clear and easy to follow step by step process of IBS from Small Intestine Bacterial Overgrowth (SIBO). IBS Treatment in Homeopathy
ReplyDelete
ReplyDeleteVery helpful post!! Followed you over here from Mugwump. Being from India I have never needed such knowledge, but you never know when things will change. Best Homeopathy Doctor in Hyderabad
IBS is now a very common health issues for all. We need give importance to all about this. You can get proper treatment for this.
ReplyDeleteibs specialist vancouver
Thank You for sharing Helpful post
ReplyDeleteMasters Homeopathy
Best homeopathy doctor near me
Homeopathy doctors near me
Best Homeoapthy Doctos in Hyderabad